Move from
“What Happened” to “Why”
Designed for Leaders Who Need to See What’s Truly Changing
In the trenches of hospital management, anecdotal concerns often drive the conversation. Focused Insights bridges the gap between data and action, providing evidence-based evaluations of your hospital’s true challenges and performance drivers, helping to:
Identify financial and clinical risks earlier.
Validate anecdotal concerns with independent data.
Enable cross-functional leadership alignment.
Make strategic decisions based on evidence.
Precision Insights for Every Hospital Audience
This is not just a report; it is a custom engagement tailored to the priorities that matter most to your team right now. We facilitate the conversation so you can focus on the strategy.
Review the hospital priorities that matter most.
Receive comprehensive executive PDF packages.
Engage in live, collaborative stakeholder presentations.
Tailor analysis for senior leadership or quality committees.

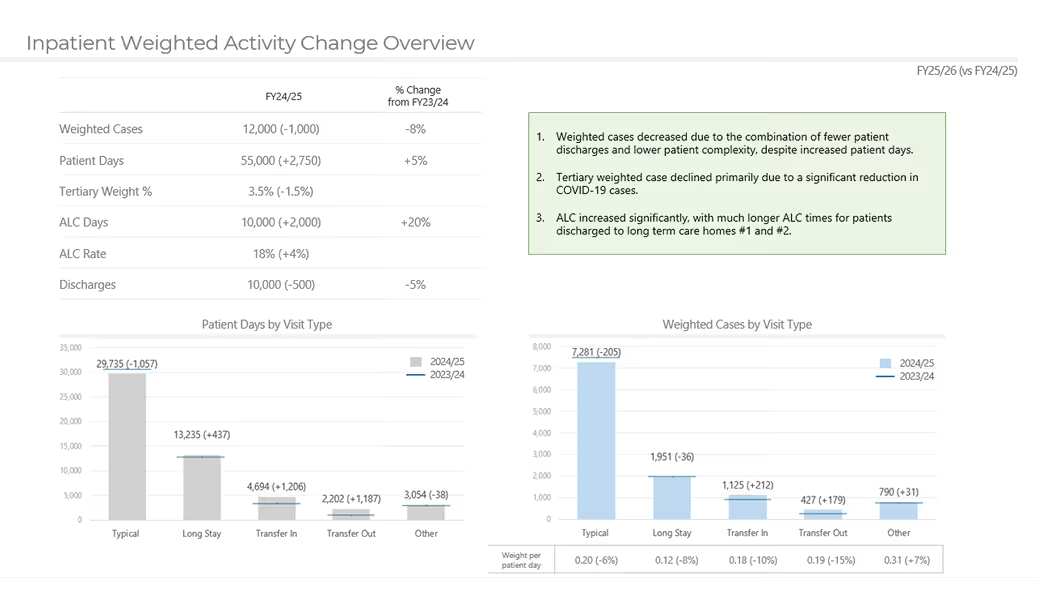
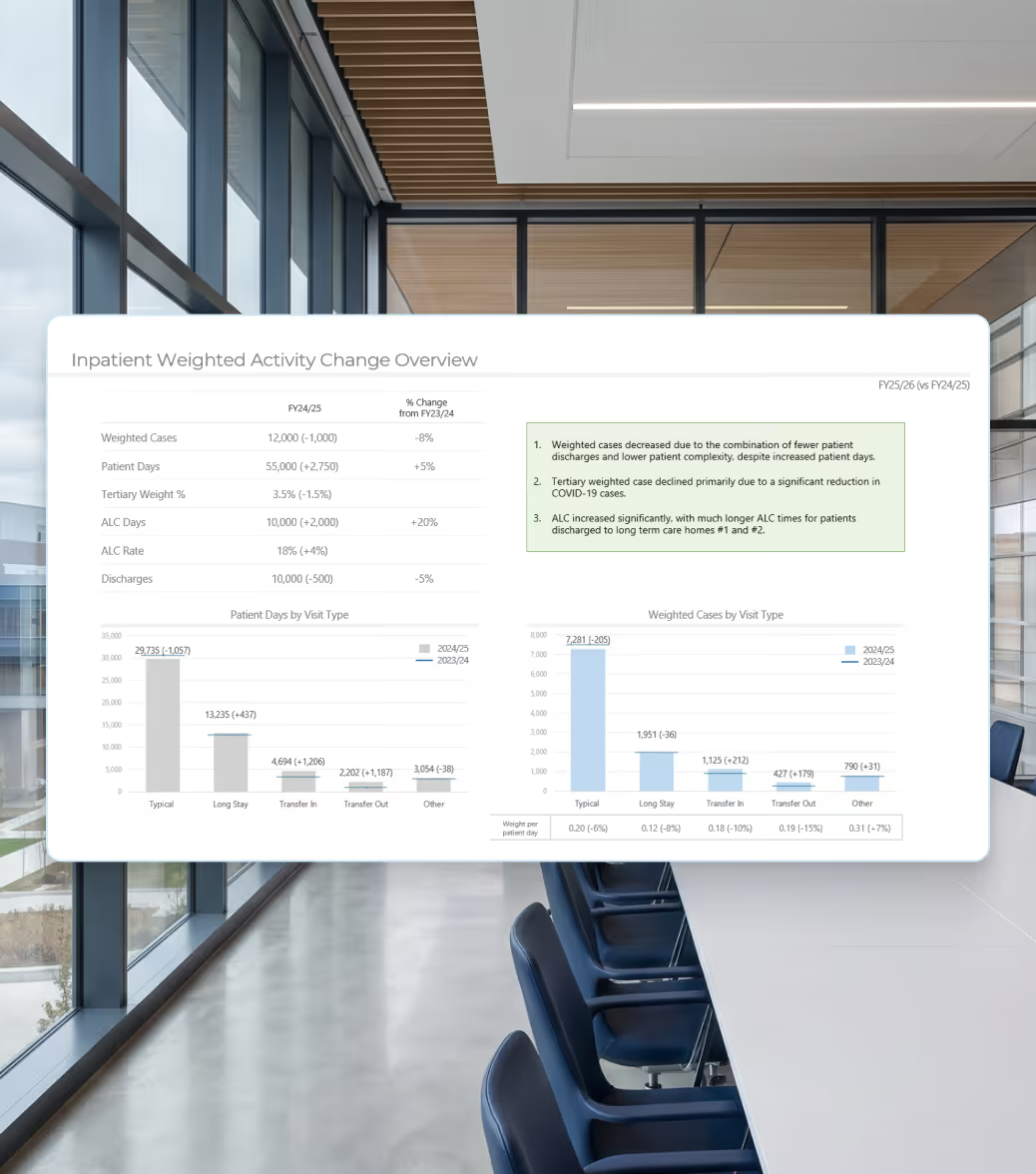
Understand the "Why" Behind Your Metrics
Instead of guessing why wait times are up or weighted cases are down, our analytics team dives deep into your specific context to pinpoint the exact drivers of change.
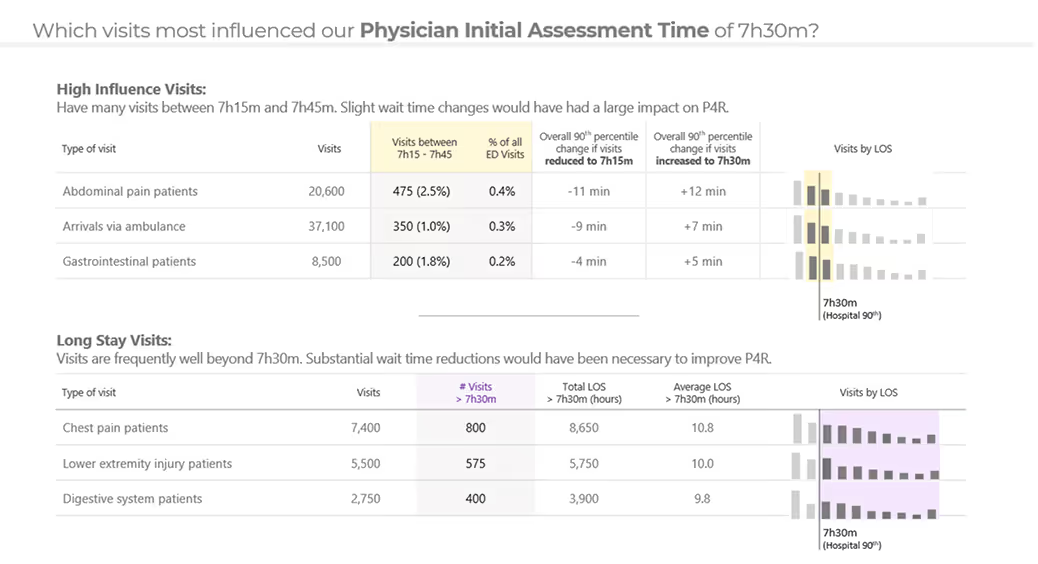
Pinpoint populations impacting ED wait times.
Identify specific factors driving weighted activity.
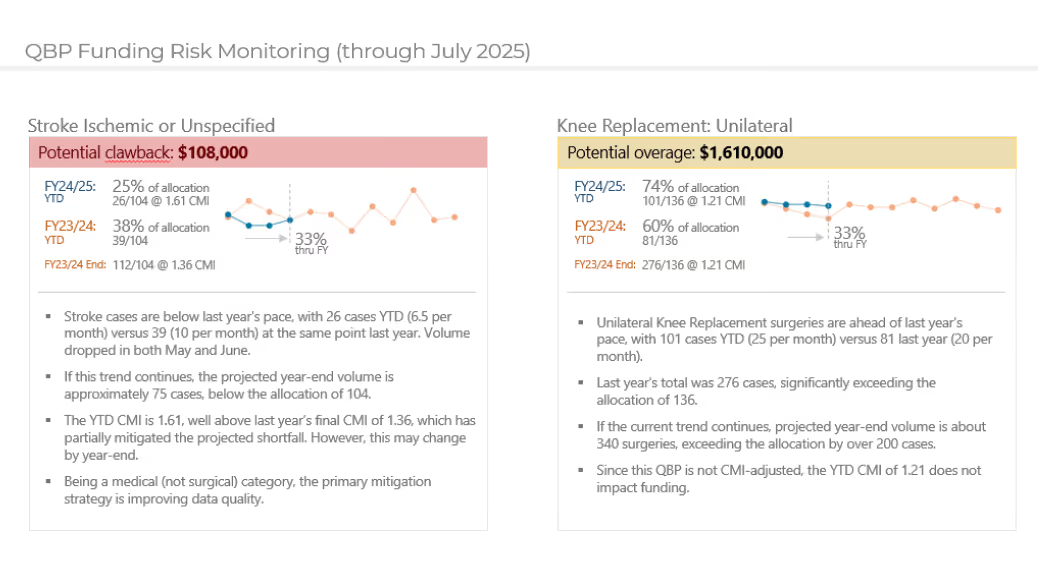
Early identification of funding risks to avoid surprises.
Understand the factors contributing to readmissions.
Support Better Decisions with Proven Expertise
Leverage over two decades of experience in the Canadian hospital landscape to launch focused initiatives that improve care quality, funding accuracy, and operational efficiency.
Reduce LOS and improve ED performance.
Support targeted clinical and data initiatives.
Quantify the impact of clinical delays and harm.
Leverage purpose-built funding expertise.
Solve Common Hospital Analytics Challenges
Focused Insights addresses the complexity that often makes hospital analytics difficult to maintain over time. We centralize logic and data into a single platform to eliminate common challenges.
Fixes indicators that are difficult to maintain as methodologies change.
Provides validation tools to reduce the risk of errors.
Eliminates data duplication across disconnected systems.
Replaces disconnected reports with a centralized framework.
Simplifies the analysis of complex patient cohorts.