Improving Data Quality Across a Multi-Site Ontario Health System
When a large Alberta teaching hospital undertook a system-wide EMR migration, leadership was concerned that reporting continuity would suffer during the transition period. 3terra's EMR Integration module was used to maintain a consistent data layer throughout the cutover, ensuring that analytics and quality dashboards remained accurate and uninterrupted from day one of the new system.

May 22, 2026
X min read

Making sense of conservable days
Conservable days represent one of hospital management's most challenging metrics: everyone watches them, few understand them, and many struggle to improve them despite significant effort. Poor performance could indicate operational inefficiency, complex patient populations, data quality issues, or methodological mismatch, and usually some combination of all four.
What are conservable days?
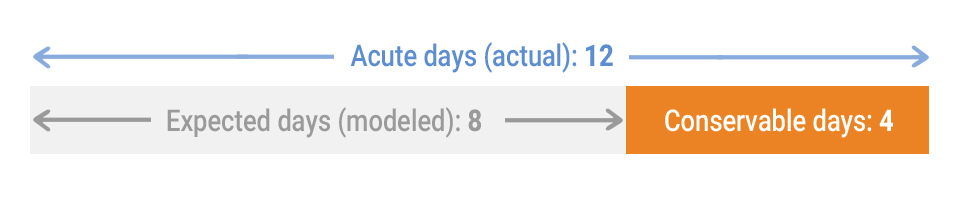
Every inpatient visit is "coded" with standardized diagnoses and procedure codes. From these codes, an Expected Length of Stay (ELOS) is calculated based on the patient's condition, age, and case complexity using CIHI case-mix methodologies and historical utilization patterns. When Acute Length of Stay (ALOS) exceeds ELOS, the difference represents "conservable days": excess days the patient theoretically should not have occupied an acute care bed.
Why are conservable days important?
Ultimately, conservable days are about better patient care. Ministries and health systems rely primarily on accountability mechanisms (funding implications and performance evaluations) to compel change. Reducing conservable days improves patient outcomes and creates capacity for others who need acute care, but only when the right problems are addressed.
- It's a widely used performance metric: Conservable days serve as an imperfect but widely used measure of hospital efficiency. Leadership is routinely evaluated on this metric.
- There are funding implications: Provincial funding models can partially fund hospitals based on theoretical bed days (ELOS) rather than actual days (ALOS), creating financial disincentives for excess length of stay.
- When used properly, it leads to positive change: Conservable days can identify care delivery problems. Tracking them to their source may reveal inefficient care paths or systemic bottlenecks that, once addressed, improve patient outcomes.
What are the main reasons for conservable day challenges?
1. Operational Inefficiencies
Operational factors can meaningfully contribute to conservable days, independent of clinical care quality. Common examples include discharge planning gaps, care coordination issues, and workflow inefficiencies such as delays in diagnostic imaging, consultant reviews, or medication reconciliation.
2. Limitations in Case Grouping Methodologies
Case-mix methodologies don't fit all hospitals equally. Complex populations create systematic distortions. Cases deemed "too long" may be reclassified as atypical and excluded from calculations, even when excess days stem from inefficiencies rather than clinical necessity.
3. Data Quality Issues
Incomplete or inaccurate coded data directly affects conservable day calculations. If visit details that increase complexity aren't captured, calculated ELOS will be lower than appropriate, artificially increasing conservable days.
Incomplete coding artificially inflates conservable days by lowering calculated ELOS. When complexity isn't captured, efficient care looks inefficient, especially in your most complex cases.
4. Conservable Day Calculation Nuances
Multiple calculation methodologies exist, each with different implications — netted vs. unnetted, case exclusions, and Ontario-specific HIG methodology vs. national CMG+ methodology.
5. Clinical Care Path Variations
Physician practice patterns vary significantly. However, attributing conservable days to clinical practice variation requires extreme caution given all the confounding factors above.
Where can data analysis help?
1. Identifying High-Impact Populations
Hospital-wide conservable day percentages often hide more than they reveal. A small number of patient groups frequently account for a disproportionate share of conservable days.
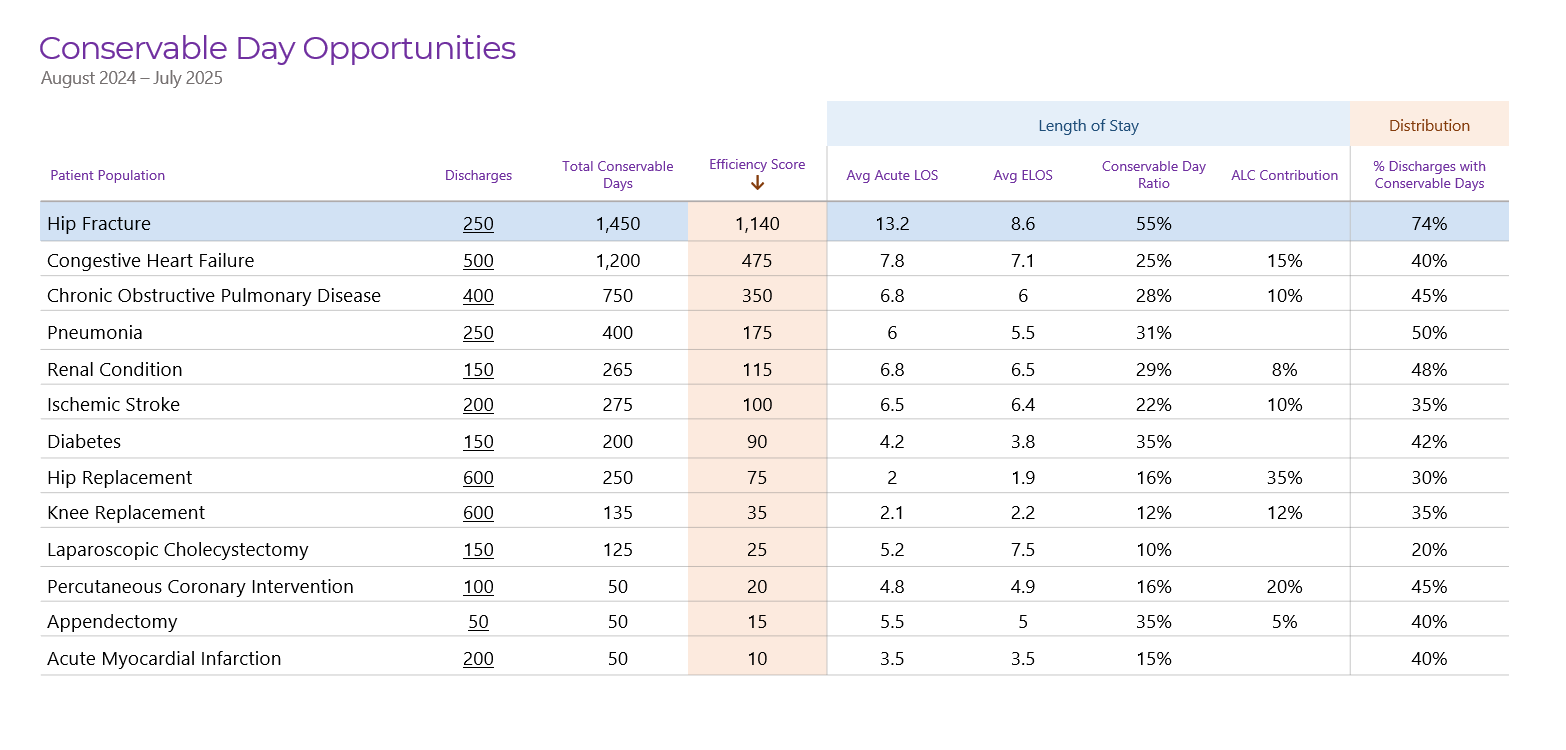
Rank patient populations by contribution to total conservable days. Look for groups with high conservable days per case along with sufficient volume to account for statistical noise.
2. Detecting Structural Discharge Barriers
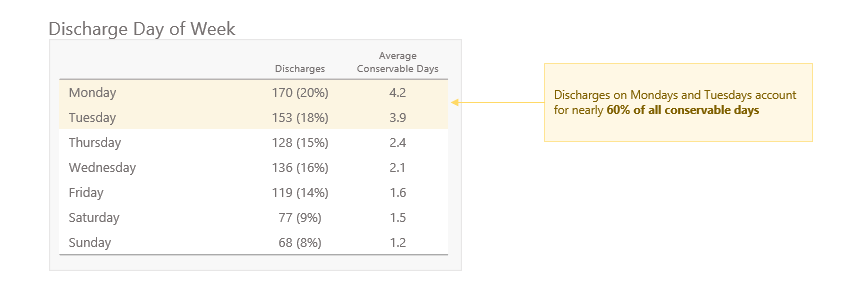
Not all excess length of stay is clinical. Patterns in the data often reveal systemic discharge friction, such as spikes in conservable days aligned with day-of-week or holiday patterns, suggesting discharge delays rather than changes in patient acuity.
3. Improving Coded Data Quality
Expected Length of Stay (ELOS) is calculated directly from coded clinical data. When diagnoses, interventions, or comorbidities are not fully captured, case complexity is understated. In our experience, data quality issues can account for up to 20% of reported conservable days.
4. Peer Comparison and Collaborative Learning
Analyzing performance in isolation makes it difficult to distinguish internal issues from broader system effects. Secure, anonymized comparison with truly comparable peer hospitals provides a more meaningful reference point than provincial averages alone.
Provincial averages mask real performance gaps. Comparison with comparable hospitals helps distinguish actual issues and enables collaborative learning and improvement.
5. Understanding Where You Are Different
Some hospitals may appear to underperform not because of poor care delivery or data quality, but because standardized calculations do not fully account for local or population-specific factors.
Some hospitals appear to underperform because ELOS calculations don't account for their patient mix. Understanding excluded factors helps you separate real issues from methodological mismatch.
Conclusion
Conservable days aren't a single problem with a single solution. Your hospital's performance may reflect discharge planning gaps, methodological limitations, incomplete coding that understates complexity, or all three. Attempting to improve without understanding this composition leads to misdirected effort.
At 3terra, we address conservable days from both angles: data quality and analytics. Our DQA platform first identifies coding gaps that artificially inflate conservable days, distinguishing measurement artifacts from genuine inefficiency. Contact 3terra to assess whether your conservable day challenges reflect data quality issues, operational inefficiencies, or both.